Hormones - Part One
[8 minute read (without links)]
Hello Thorny Roses! Let’s have a quick delve into the topic of hormones, shall we? It is, after all, pretty crucial to women, of all ages, but of particular pertinence when it comes to the perimenopause and menopause.
Where are you with this? Are you still cycling? Entering into the perimenopausal phase? Fully menopausal/post menopausal? What are your views on hormones? And have those views changed over time? Do you have a condition that precludes taking hormones, estogen in particular?
Whatever your experiences or feelings around them, there’s no doubt that hormones are immensely powerful. You might recall that they are described as “chemical messengers”, and there’s something in that phrase that suggests the messages could just be ignored. That the Queenly brain could listen to the message and decide whether or not to act on that information. It’s really not like that. The messages are instructions, and ignoring them is not an option. Hormones don’t just exert a bit of an influence on how we feel and act, they are to a large extent the instruction manual.
I just want to untangle some of the issues and considerations around all of this. Some of these sometimes get missed out of the discussion, and I believe they are crucial to consider.
The Symptoms are the problem but they aren’t the whole problem
Let’s quickly re-cap what’s going on:
The sex hormones have a job to do around reproduction, releasing eggs, preparing the womb for implantation, maintaining pregnancy, enhancing desire, and so on. It’s a complex symphony, with each phase triggered by the previous phase, with different outcomes depending on whether or not an egg is fertilised. As women get older, and towards the end of their supply of eggs, there are some months when an egg isn’t released. This means the next movement isn’t triggered in the same way, the hormones are out of balance, and various symptoms ensue - especially those around temperature regulation (night sweats and hot flushes), but there are plenty of others as well, including weight gain, heavy periods, fatigue, vaginal pain, brain fog, rage and vile moods, sleep disruption, headaches and migraines, depression, anxiety, joint pain, low libido, heart palpitations, bleeding gums, hair loss, hearing loss and tinnitus, increased gas, burning tongue, formication (a feeling of crawling on the skin), muscle pain, light-headedness, dizziness, breast tenderness, pins and needles in the extremities….. Blimey, what a list and that isn’t even everything! Thanks, perimenopause! This phase of irregular cycles and unbalanced hormones can last for several years, but the body is on a downward trajectory in terms of making the sex hormones. Generally, once these have plateaued, a fair number of the troublesome symptoms will have stopped.
So if women do nothing at all, a lot of their symptoms will resolve over time.
But there are a few things to consider here.
For some women, the symptoms are so debilitating that doing nothing at all isn’t really an option.
But here’s the other thing that is really worth thinking about carefully, and which doesn’t necessarily get addressed when just considering the unpleasant symptoms such as hot flushes.
The hormones progesterone, estrogen, and testosterone had more jobs to do than just regulating the menstrual cycle, and whilst the imbalance was a wild ride, the calm that comes after that storm is not necessarily the best place to be. Which is to say, you might not be having hot flushes anymore, but the issues that arise from massively reduced amounts of these important hormones (such as bone and muscle loss) still need to be addressed.
Let’s look first at what these hormones do for us, and the impact that low levels of them can have.
Progesterone
The benefits of progesterone are many. Known as the calming hormone, it helps sleep, enhances mood, and reduces anxiety.
It also protects the brain (has been described as a neurosteroid), and can reduce debilitating brain fog.
It provides pain relief, is anti-inflammatory, increases connective tissue stability, and is also involved in bone and muscle health.
It helps with energy, keeping weight down, temperature control, hair growth and protects against anxiety, depression and more.
Finally, it helps with “vagal tone”, a marker of how well your body can relax after stress.
For more detail on some of these points, there’s a good article by Nicki Williams on LinkedIn here:
Estrogen. We produce three kinds of estrogen throughout our lives. Estradiol, E2, is the most potent form, that we have during our potential reproductive years, produced by the ovaries. Estriol is produced during pregnancy, and Estrione is what we produce after menopause, created in the adrenal glands and in fatty tissue. It is this that makes belly fat “active fat” and the need for this hormone production is part of what gives rise to what some people call “ menopot”, a characteristic fat distribution that is very resistant to attempts to change it. Little wonder, since it’s doing an important job beyond simple energy storage.
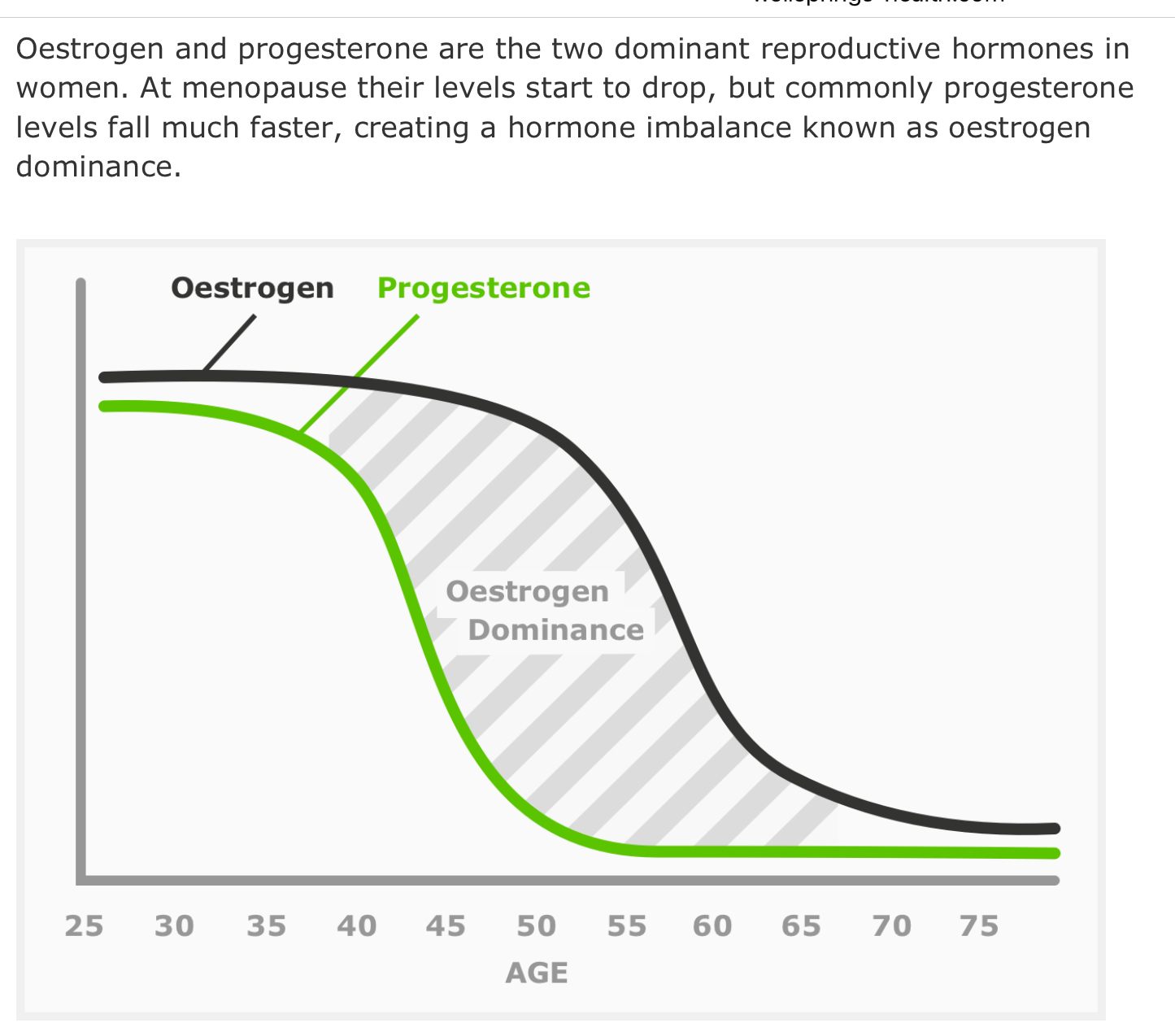
As mentioned earlier, part of the issue is that as E2 estrogen levels decline, it leaves important jobs undone, but also the decline is non-linear meaning that it doesn’t reduce at the same rate as progesterone, and that imbalance is a big part of the problem.
But what jobs does E2 do, outside of cycle management?
It promotes muscle growth and strength, critical as we age and lose muscle anyway.
It supports mitochondria function, allowing fuel to be turned into energy for our activities
It regulates systemic inflammation, thus reducing joint and muscle pain.
It manages blood sugar, and regulates appetite.
It manages moods, by increasing serotonin, and controlling cortisol.
It controls body temperature, by managing control mechanisms such as blood flow to the skin and swearing.
It controls blood pressure, helping the constriction and dilation of blood vessels, keeping their “tone” high.
Assists in building bone, by increasing calcium absorption and regulating key mechanisms involved in maintaining bone turnover and density.
And it’s good for vaginal health, too!
Testosterone:
We don’t produce a lot of testosterone compared to men, but it still has an important role, in conjunction with estrogen and progesterone, in maintaining healthy bones and muscles, protecting our brains and firing up our sex drives. We still produce it, via ovaries and adrenal glands even after the other hormones have declined, but sometimes not in sufficient quantities. It isn’t something prescribed on the NHS, however. For some women, it has been the missing piece of the jigsaw but they have had to go private to get it.
Looked at like this, it’s no surprise that fluctuating and declining levels of these hormones can have such a disruptive effect on so many areas of our lives.
There are three principle ways of dealing with the issue.
“Naturally” - using supplements, adaptogens, exercise, healthy lifestyle approaches, phyto estrogens, vitamin supplementation to increase natural production, and so on.
Hormone therapy- to add back into the body the hormones it is no longer producing or not producing very much of
A combination of the two.
Each woman will come to her own decision, of course. And in the next articles we’ll look at some culturally pervasive myths and attitudes that are out there, as well as how hormone therapy and other approaches work. But before we do, there’s something I’d like to point out:
Women often hit perimenopause already depleted
This is something I don’t think we take into consideration enough. The rollercoaster assault on our bodies and minds that wildly fluctuating hormone levels inflict would be challenging enough if we were well rested, well supported, well nourished and able to take the time we needed for ourselves, dropping our commitments to just the bare essentials and going deeply into self-care and being cared for by others within a loving community of wise women and supportive men, within a society that appreciated and valued us as women in all the phases of our lives. Sorry, got a bit carried away there. Instead….
By the time we get to this phase in our lives, we have often experienced quite a number of the following (this is like those “never have I ever” quizzes on social media where you get a point for each crazy thing you have done, but in this case you would want your score to be low….):
Having an exhausting job or two, or three
Mothering teenage kids, possibly as a single or primary parent
Not mothered anyone, and mourned that loss
Looking after elderly parents
Going through a divorce/separation
Suffered a bereavement, or several
Struggled with financial worries
Carrying the mental load
Doing more than our share of work
Having had or still experiencing disordered eating
Having had or still experiencing mental health issues
Been sexually assaulted
Been pregnant
Had a miscarriage
Had a termination
Had an unpleasant medical procedure
Been over/under weight
Been bullied at work
Lost a job
And so on and so on
My point is that many of us hit perimenopause already depleted, with few resources both within themselves and within society. Depleted and stressed. And stress itself has an impact on our levels of progesterone, and a negative effect on just about every aspect of our health. Some of us will go almost straight from having babies into perimenopause. Others will find themselves facing fluctuating hormones at the same time their daughters hit puberty. We might be caring for elderly relatives and have demanding jobs. We are likely to be the ones holding it together, carrying the mental load, feeling like we are still the ones in charge of everything but finding the strain of doing that whilst in the depths of brain fog to be almost impossible. Many perimenopausal women fear they are suffering early dementia, because their ability to think straight and remember things is so badly affected. We live in a society in which taking time for self care is seen as deeply selfish, and where we praise over-commitment and extreme achievement above much else. We also live in a highly industrialised society and much as we know that in some cultures women have a much easier time of this transition, that can seem like an additional pressure on us (why can’t we be more like the Japanese?), and also lead to women from those cultures not being taken seriously when they do experience difficulties.
For some of us that grew up in the 60s, 70s and 80s, the feminism of the time focussed quite a lot on proving our worth, and on minimising the challenges that women faced, as a push back against the prevailing view that “women can’t [do this important job] because period pains make them unreliable/having babies takes them out of the career path/their physiology makes physical work more difficult for them.” Rather than saying: “women face these additional challenges, but since they do such valuable work [allowing the continuation of the human race, and being a valuable creative force with wisdom, knowledge and skills to offer], let’s ensure that working practices/office design/healthcare services allow them to participate fully and without detriment to themselves”, the prevailing attitude was: “if women can’t be more like men, they shouldn’t be in the workforce at all, except in a few roles uniquely suited to them”. It’s even a little telling that I chose to emphasise the value women bring, and that therefore we “deserve” accommodations, rather than that adjustments should be made anyway, because of the challenges, full stop.
I think it’s partly due to this heritage, and the fact that these opinions still exist, that women often don’t speak about menopause, won’t “admit” to being in it, and won’t ask for accommodations. At work (at a one-to-one Personal Training Studio) the owner was a little taken aback at a female clients’ unwillingness to take a relatively early morning slot. I think he thought she was being a “difficult woman” (and I refer to Jane Goodall’s point here!). She pointed out that as she often didn’t sleep well at night, the hours between 5am and 10am were often prime sleeping hours for her and she tried to avoid commitments at that time. Bravo. This is the sort of thing that could make working life easier for perimenopausal women.
There are plenty of things that partners could do to make life easier as well.
Looked at like this, it’s little wonder so many women find this phase of their life so challenging. It doesn’t have to be like that, however, and there’s lots we can do to alleviate or eliminate the symptoms and perhaps find a new way forward into what can be a liberating phase of a woman’s life.
More on that in the next articles.